
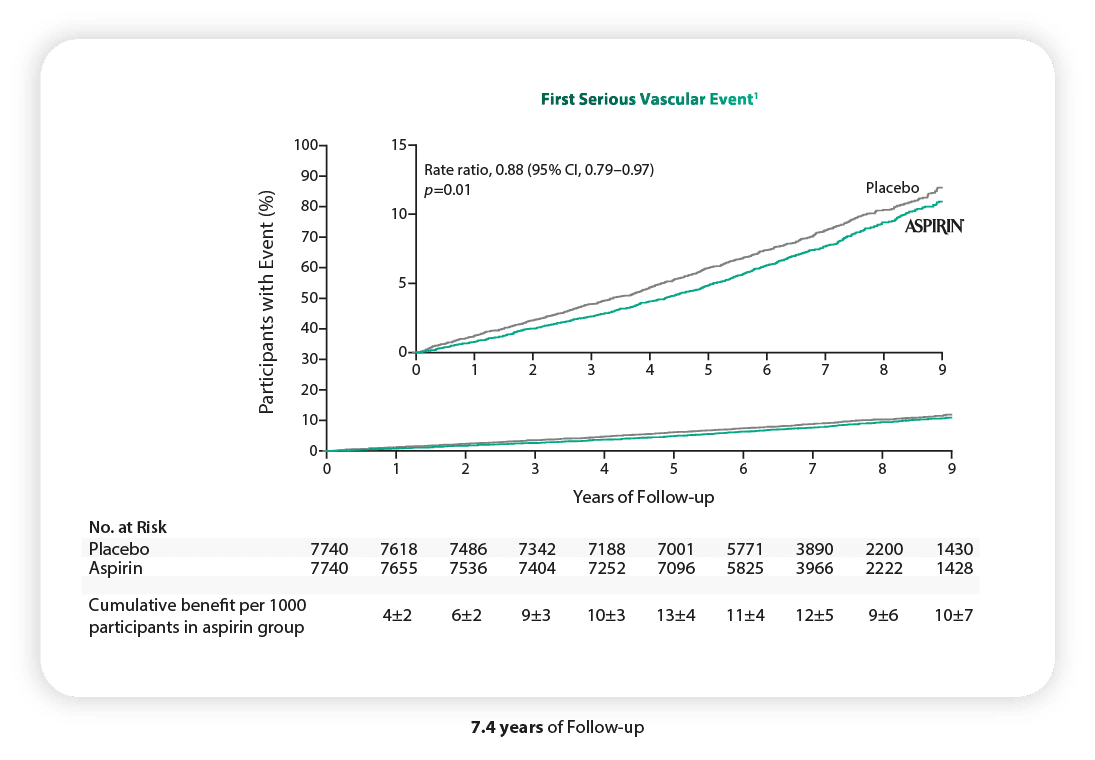
The use of low-dose aspirin led to a lower risk of serious vascular events than placebo, p=0.01.
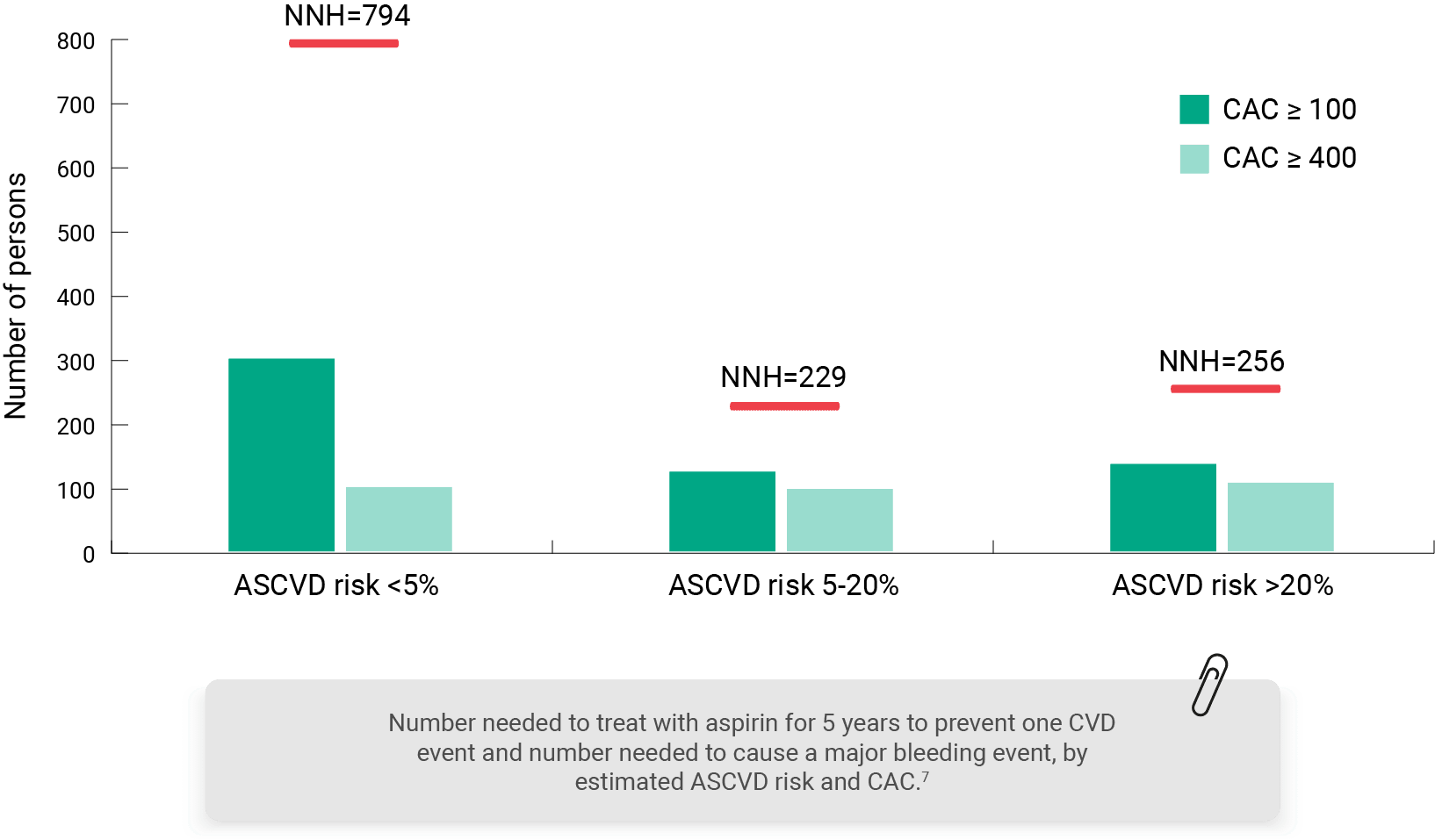
Aspirin use for 1ry prevention of CHD had favorable risk/benefit estimates in patients with CAC ≥100 and CAC ≥ 400.6
The red horizontal lines represent the NNH threshold for each ASCVD risk stratum.
In a sample of >11 000 US adults- who were not taking aspirin and were free of high‐risk bleeding features-NNT5 to prevent 1 ASCVD event with aspirin was approximately 50% to 70% lower among individuals with prevalent or moderate carotid plaque (CPS ≥2) versus absent carotid plaque (NNT5 = ≈150–212 versus 448).
As reflected in recent guidelines, the approach to using aspirin as primary prevention therapy is continuously evolving and requires personalization; therefore, there is an urgent need to identify the patients who are most and least likely to derive net benefit from daily aspirin therapy.
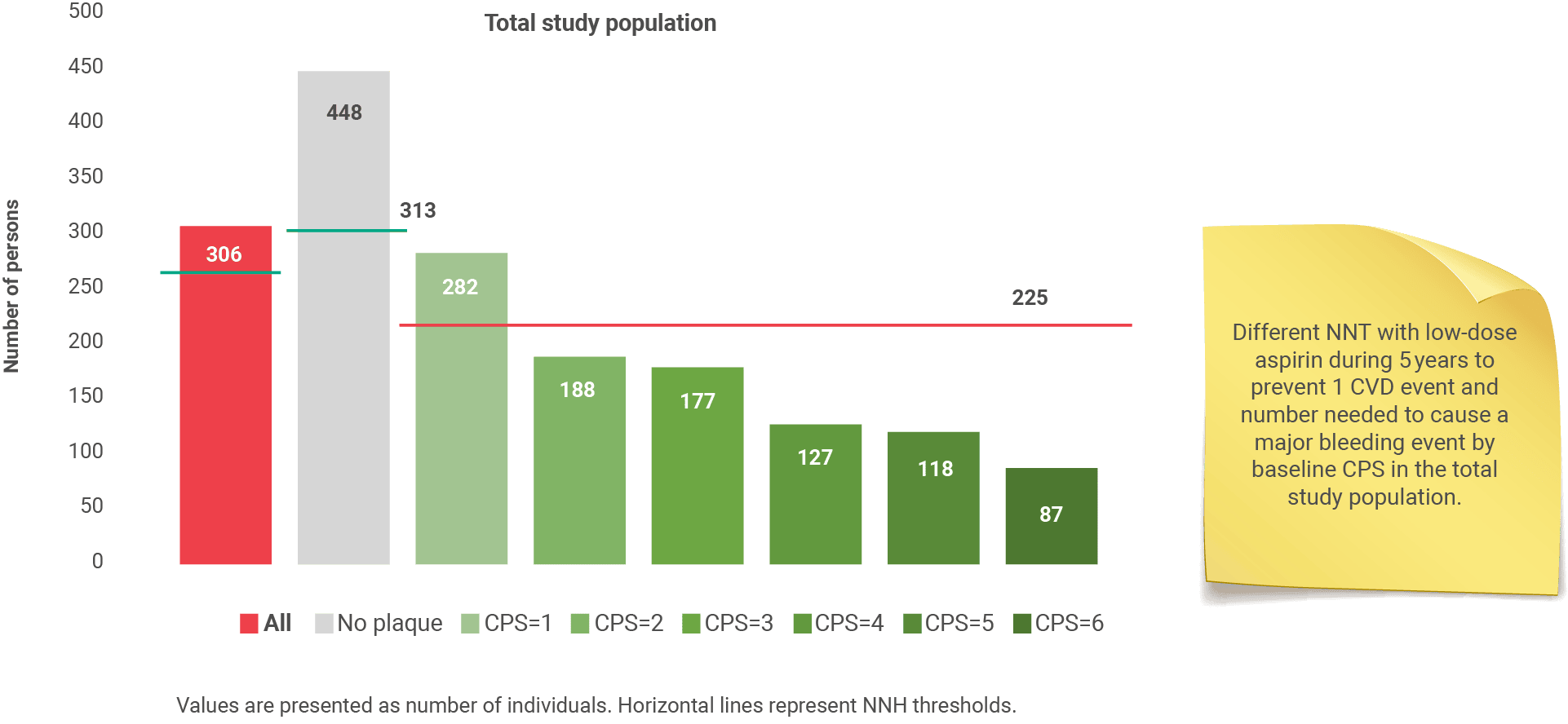
ASCVD: Atherosclerotic cardiovascular disease; CVD: Cardiovascular disease; MI: myocardial infarction; CAC: coronary artery calcium scoring; NNH: number needed to harm; CPS: carotid plaque score; NNT: number needed to treat.
References