
Aspirin 100 mg adequately suppresses platelet activation in type 2 diabetic patients irrespective of their glycemic control and comparable to the effect in healthy subjects1
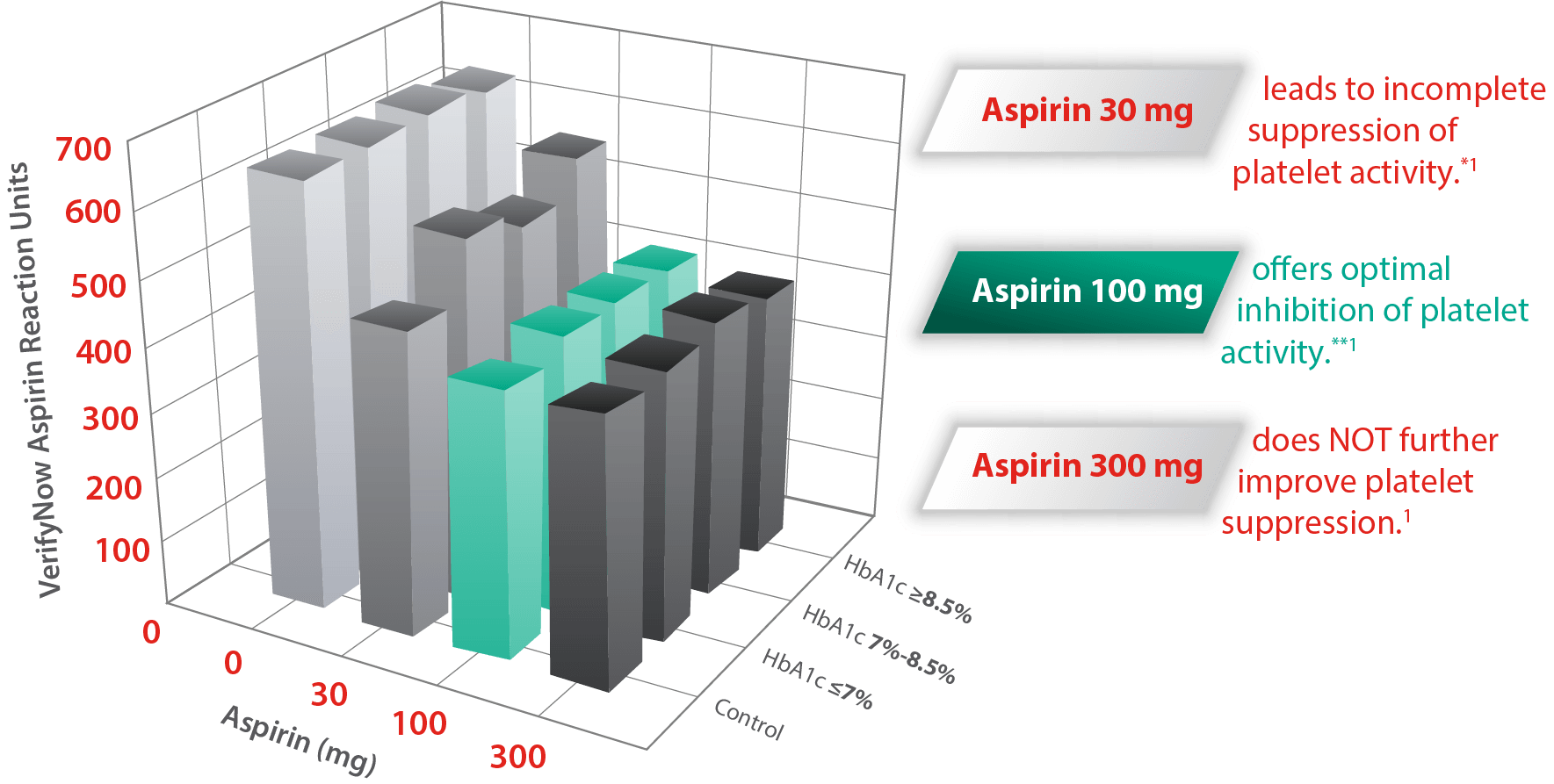
*Especially in patients with poor glycemic control.
**Irrespective of glycemic control.
Aspirin 100 mg adequately suppresses platelet activation in type 2 diabetic patients vs. incomplete suppression with 30 mg, and no additional benefit with 300 mg dose.1
Using different doses of Aspirin
showed that daily doses <75 mg seemed to have a somewhat smaller effect2
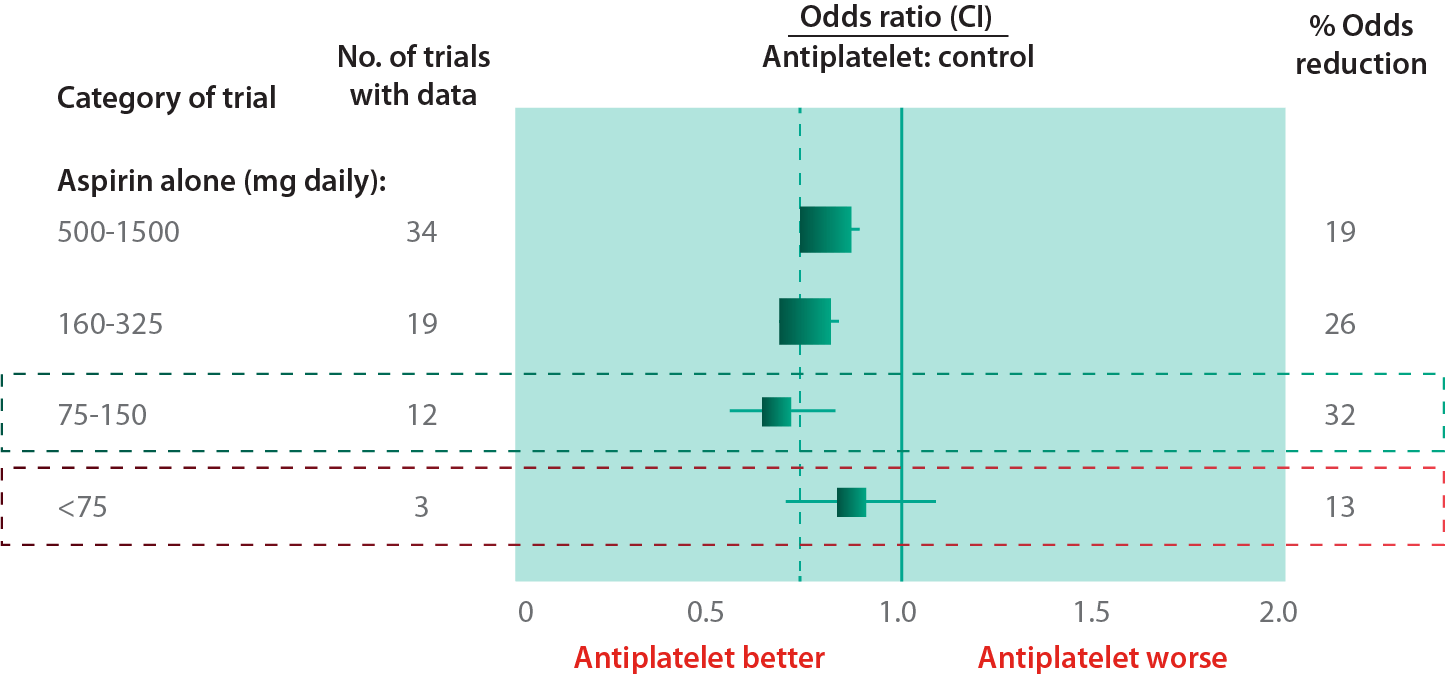
A meta-analysis of several trials using different doses of aspirin showed that daily doses <75 mg seemed to have a somewhat smaller effect with proportional reduction 13% (p=0.05). 2
162 and 325 mg aspirin significantly reduced urinary 11-dh-TXB2 levels compared with 81 mg aspirin in diabetic patients3
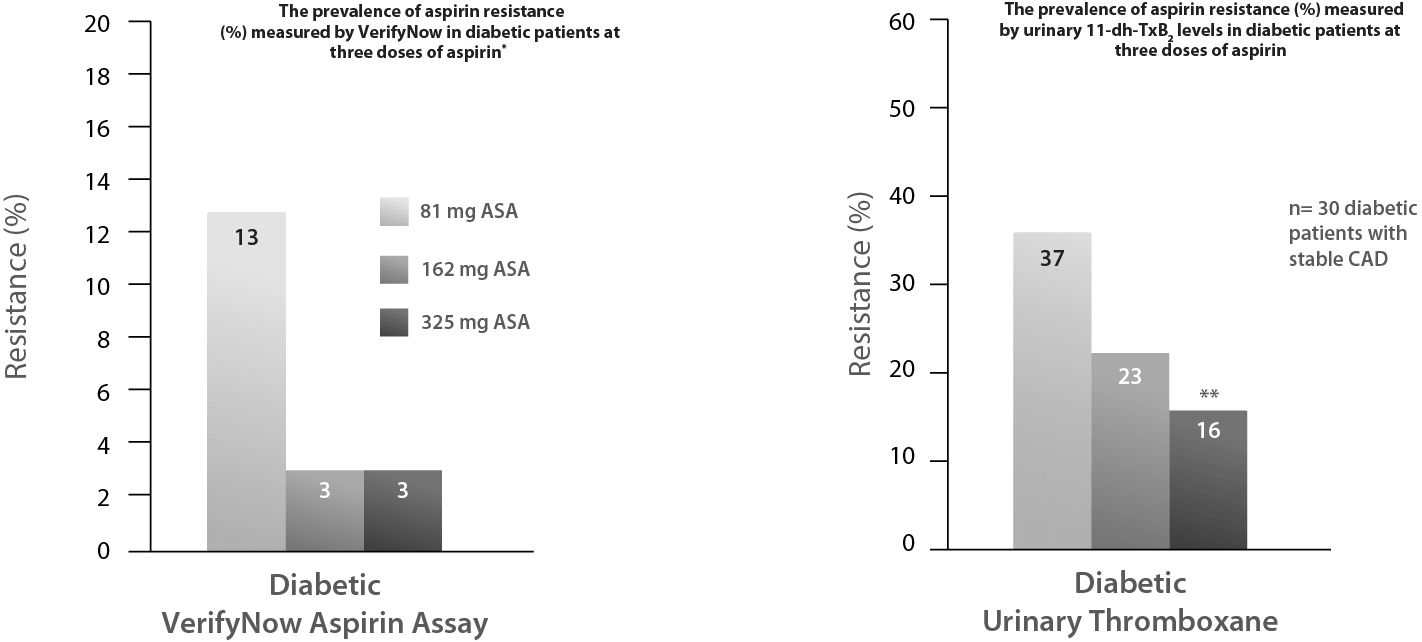
The ASPECT study showed that 162 and 325 mg aspirin significantly reduced urinary 11-dh-TXB2 levels compared with 81 mg aspirin in diabetic patients (p=0.01 and 0.002, respectively).3

*Directional trend in reduced rates of aspirin resistance was observed in diabetic patients with doses >81 mg (p =0.16); however, rates of resistance in nondiabetic patients were uninfluenced by increased aspirin dosing. Low-dose aspirin therapy may not provide adequate platelet inhibition in selected diabetic patients and that higher aspirin dosing reduces the prevalence of outliers above the cut points for resistance.3
**p≤0.05 for difference in resistance between 81 and 325 mg aspirin within the group of diabetic patients.
ASA: acetylsalicylic acid; CAD: coronary artery disease; WHO: world health organization.
References