
Unlike the risk factors-based scores which rely on the probabilistic calculations derived from population-based studies, cardiovascular imaging techniques allow for direct visualization and quantification of subclinical atherosclerosis for a more accurate, personalized risk assessment and treatment approach.1
Coronary artery calcium scoring is a non-invasive imaging test that uses a CT scanner to measure the amount of calcium in the walls of the coronary arteries.2
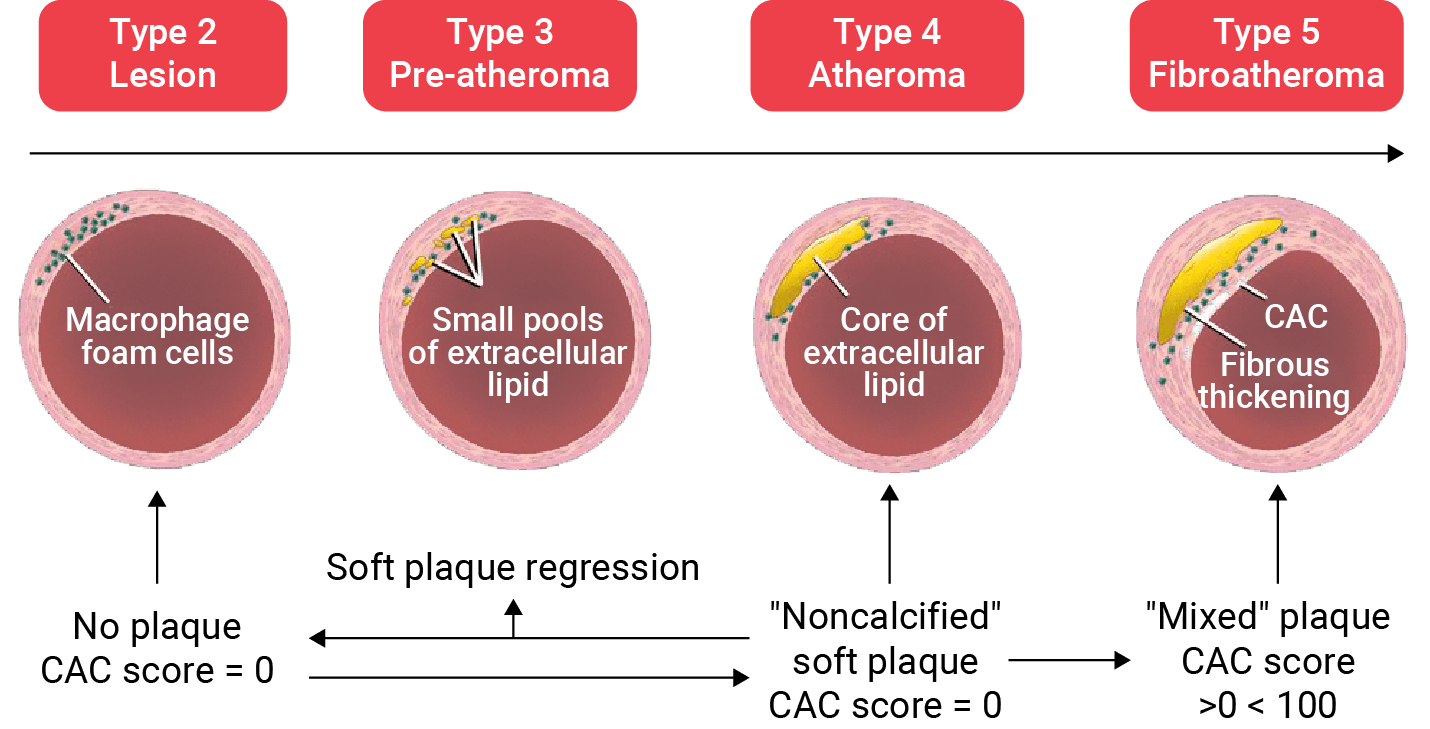
CAC is a reliable marker of coronary atherosclerosis and vascular age. Thus, CAC is useful for assessing risk and predicting future atherosclerotic cardiovascular disease (ASCVD) events in asymptomatic patients with no established coronary artery disease.3
The presence or absence, amount, and distribution of CAC are strong prognostic indicators that can assist physicians in reclassifying patient risk status as necessary.3
More than 50 % had been categorized as low risk just before the event (in an examination of 1,475 people who had a myocardial infarction before or at age 50).4
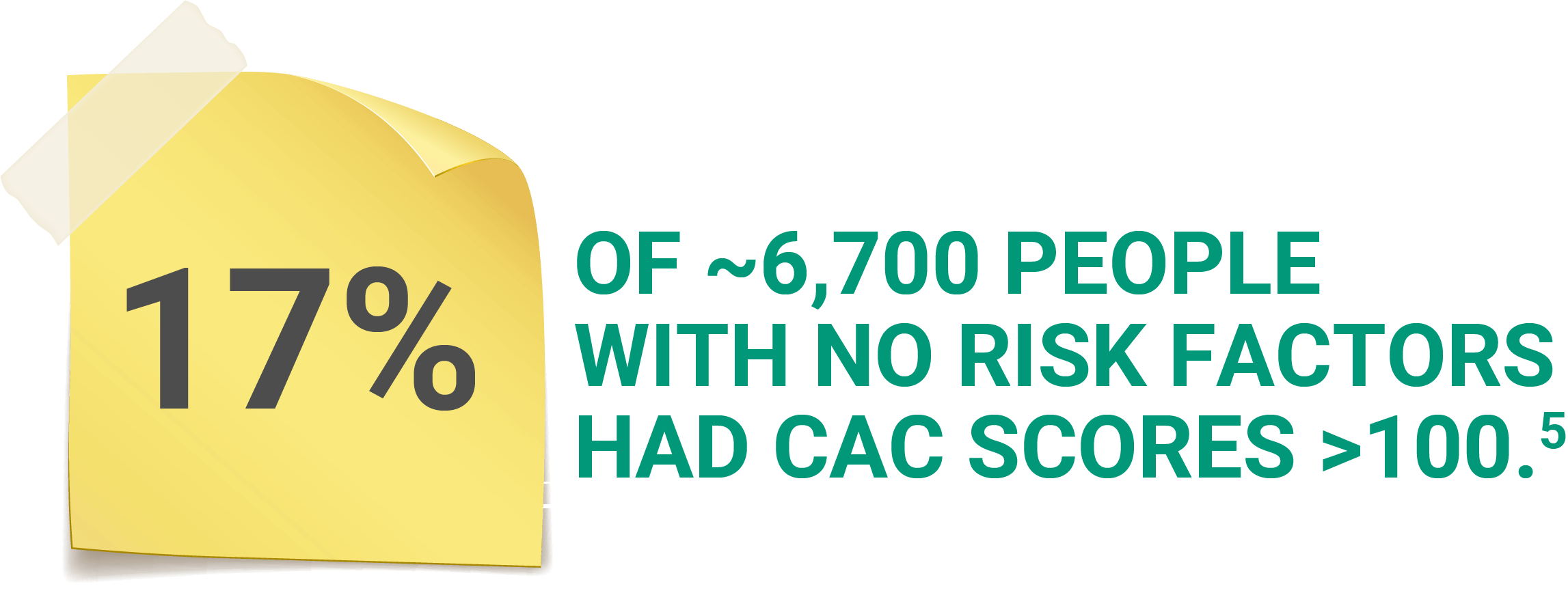
Many studies have revealed that many coronary events occur in people who were not previously considered high-risk, do not have known obstructive coronary artery disease, and/or have normal functional tests.4
CAC scores could be used as reliable gatekeepers for risk classification and the initiation of preventative therapies.6
In the absence of a high bleeding risk, aspirin is likely to be effective in those under the age of 70 who have a CAC ≥ , and they have an absolute net benefit from using it.7
CAC scoring is a robust marker of coronary atherosclerotic plaque burden and can be used to determine the need for and intensity of preventive therapies.8,9
| Agatston score | Plaque burden | Probability of significant CAD |
|---|---|---|
| 0 | No plaque | Very low |
| 1-10 | Minimal plaque | Low |
| 11-100 | At least mild atherosclerotic plaque | Mild or minimal coronary artery stenosis |
If CAC scoring is inaccessible or not feasible, a carotid artery ultrasound can be used to predict CVD events by measuring carotid intima-media thickness or assessing carotid arterial plaques.11, 12
Cost-effectiveness: low-income countries can utilize arterial ultrasounds to identify at-risk individuals.11, 12
Low-income individuals are less likely to be screened for CVD or receive preventive care than high-income individuals that reside in the same country regardless of existing CVD status.11, 12
Measurement of carotid intima-media thickness (CIMT), CIMT measurement identifies areas of increased carotid artery wall thickness, providing an easily accessible imaging biomarker for the classification of cardiovascular risk for individuals as well as population cohorts.10
Assessment of carotid arterial plaque, a sub-intimal process, may be more reflective of atherosclerosis, as it correlates with overall atherosclerotic burden in the coronary vascular bed. The assessment of carotid arterial plaque offers an even greater risk stratification benefit than CIMT.10
2x increase in death rate from IHD and other vascular causes for each 20/10 mmHg rise in BP in some age groups, starting at 115/75 mmHg.13

The overall reduction of about one fifth per mmol/l LDL-C reduction is translated into 25 fewer participants having major vascular events per 1000 participants without pre-existing MI or CHD at baseline.14
Association of a small dose of aspirin with active antihypertensive treatment reduced the risk of acute myocardial infarction without exaggerating the risk of cerebral bleeding.15
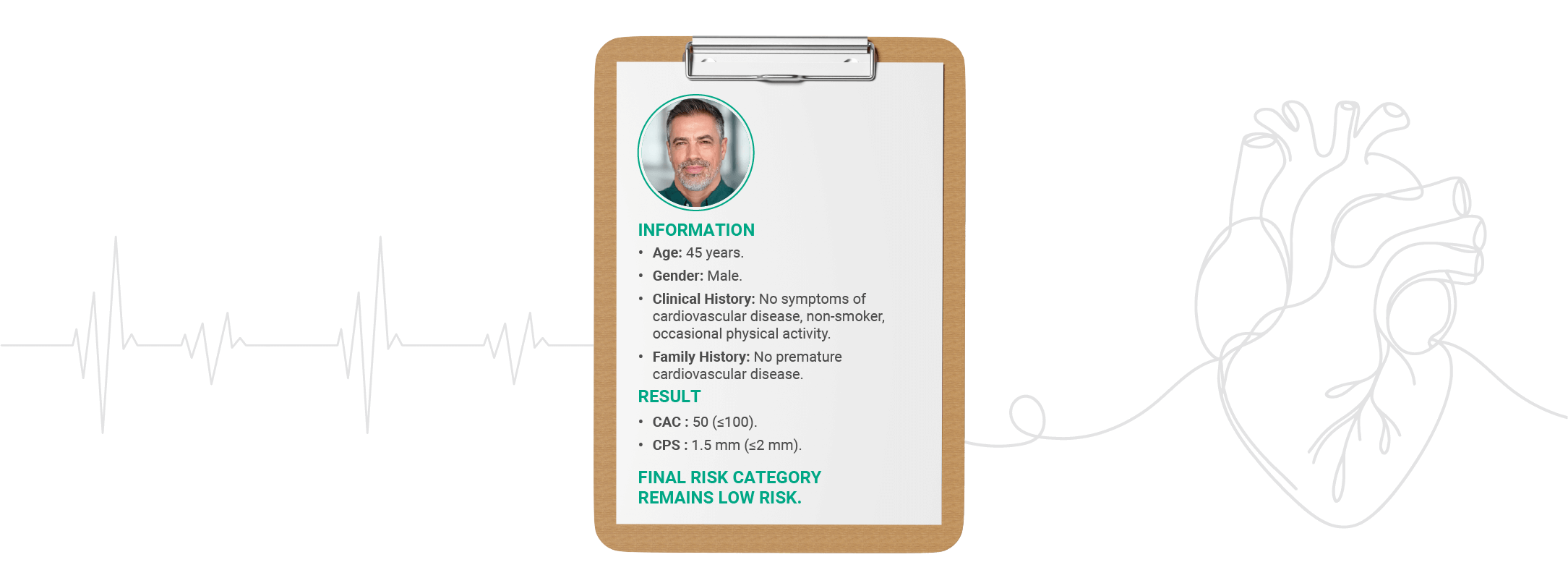
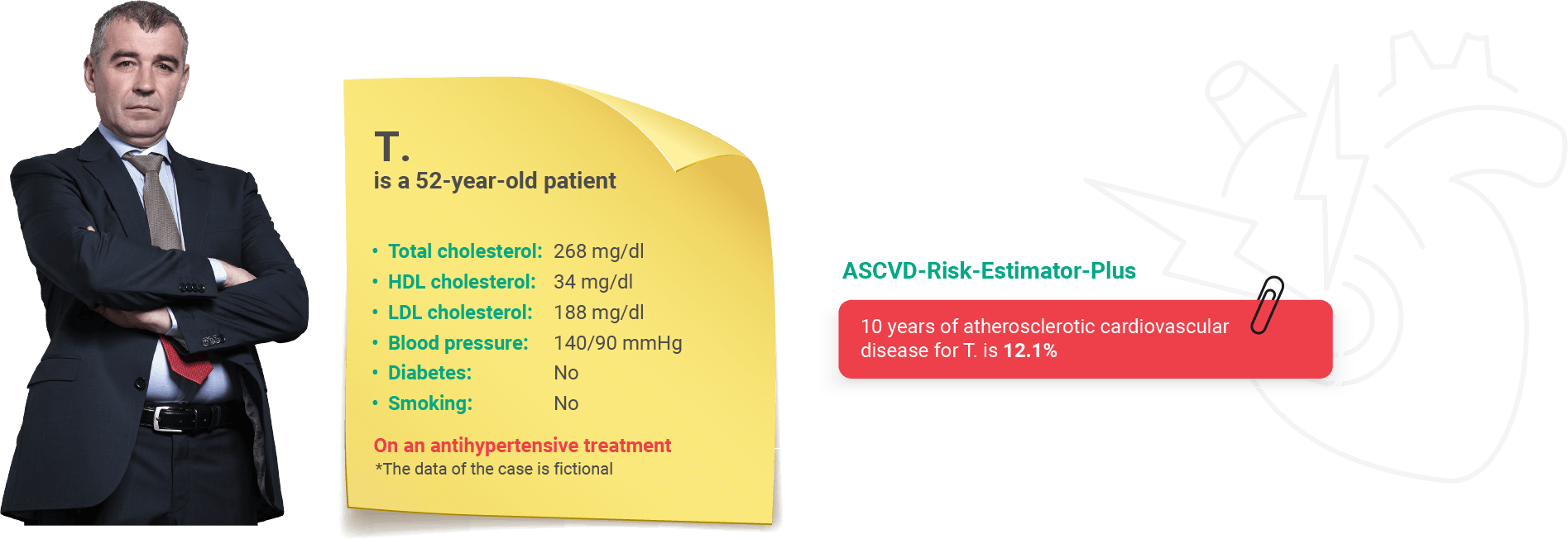
T. is at intermediate risk, he needs CAC & CPS

2x increase in death rate from IHD and other vascular causes for each 20/10 mmHg rise in BP in some age groups, starting at 115/75 mmHg.13
The overall reduction of about one fifth per mmol/l LDL-C reduction is translated into 25 fewer participants having major vascular events per 1000 participants without pre-existing MI or CHD at baseline.14
RR of ischemic heart disease death in diabetics vs. nondiabetics is 1.8 (men); RR of ischemic heart disease death in diabetics vs. nondiabetics is 3.3 (women).15

The use of low-dose aspirin leads to a lower risk of serious vascular events.16
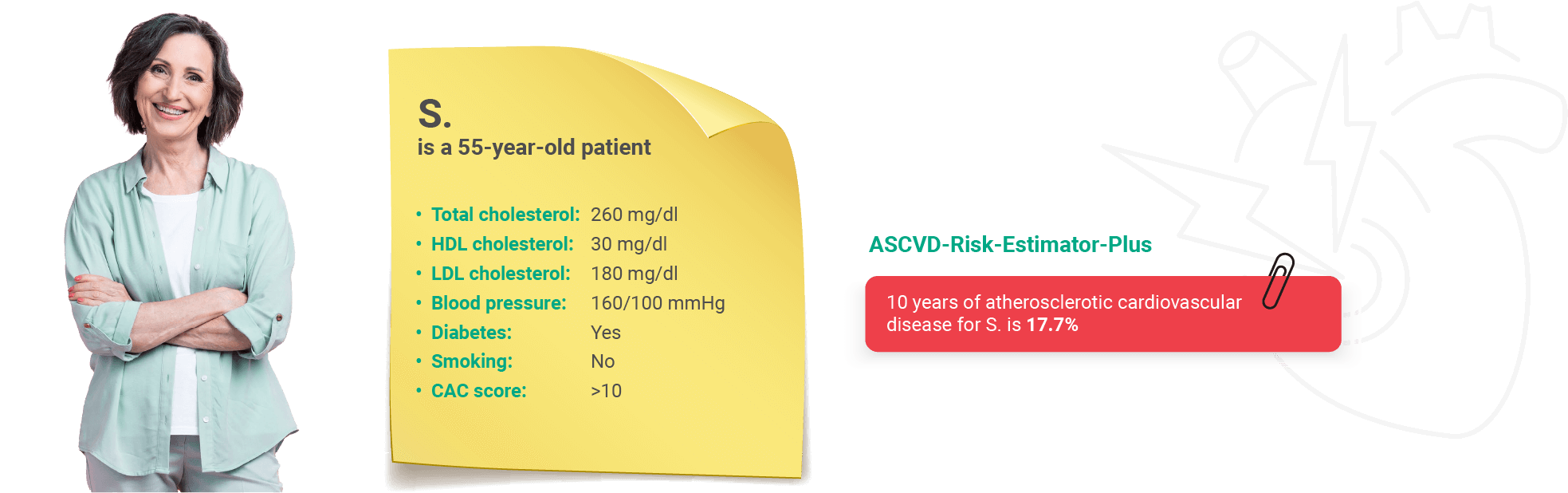
S. is at intermediate risk, she needs CAC & CPS
CAC: coronary artery calcium; CVD: cardiovascular disease; CIMT: carotid intima-media thickness; CAD: coronary artery disease; HDL: High-density lipoprotein; LDL: Low-density lipoprotein; BP: Blood pressure; LDL-C: Low-density lipoprotein cholesterol; MI: Myocardial infarction; ASCVD: Atherosclerotic cardiovascular disease; IHD: ischemic heart disease; CHD: coronary heart disease; RR: relative risk; CPS: carotid plaque score; NNH: number needed to harm; and NN: number needed to treat.
References